Swallowing Mechanism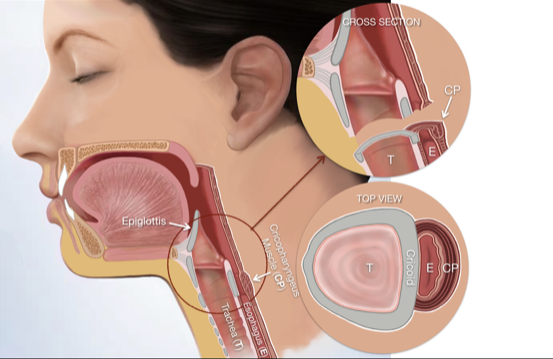
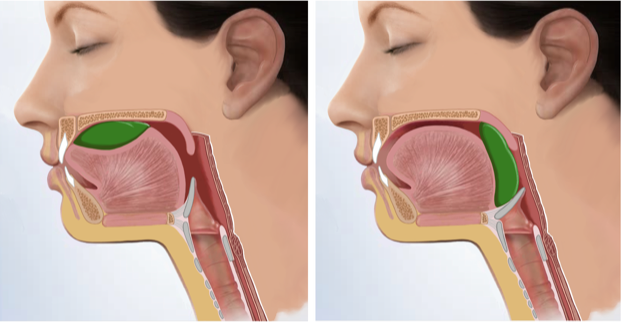
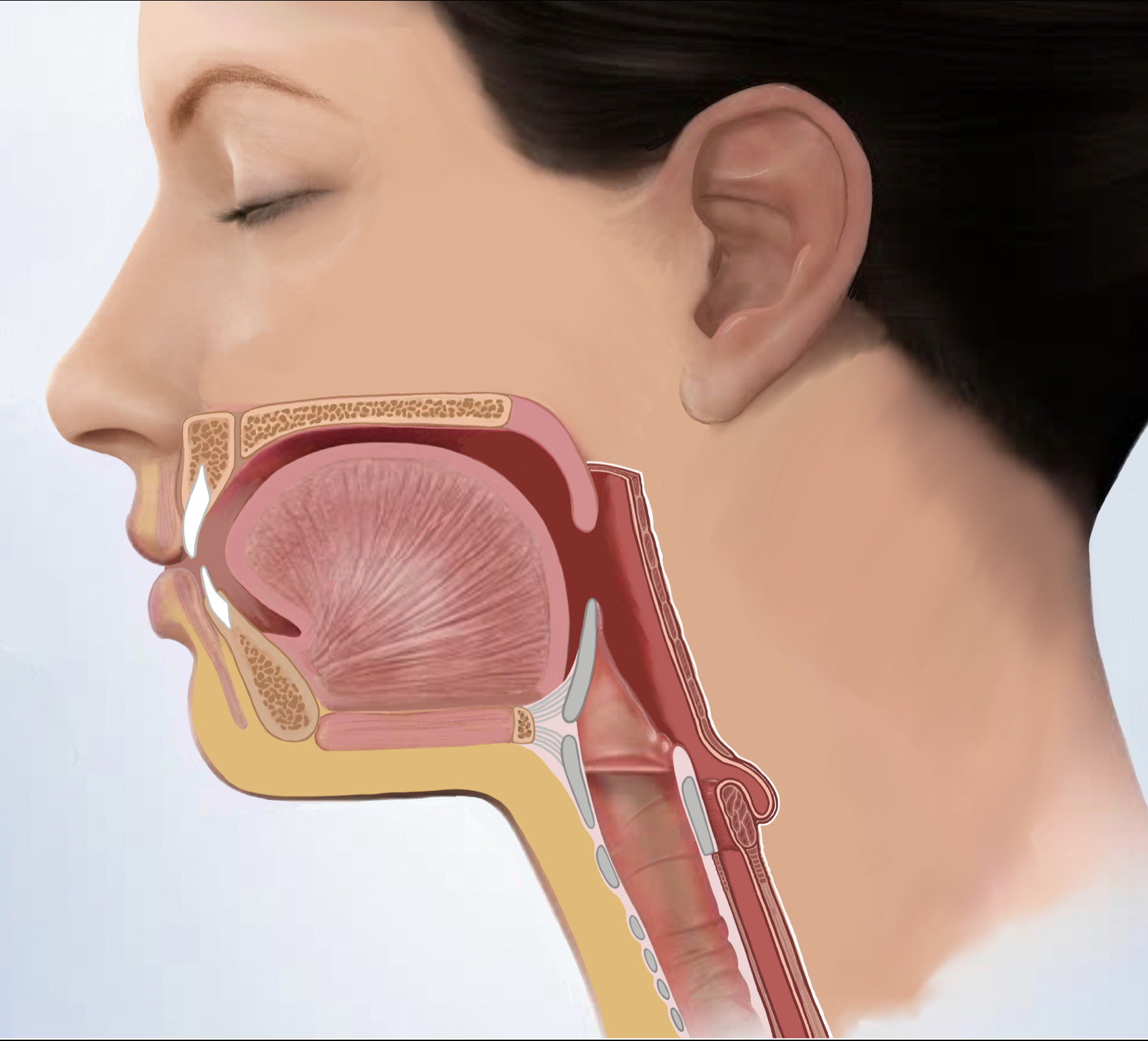
To understand swallowing issues, it is best to know the basic anatomy and physiology of swallowing (Figure 1). The mouth essentially grinds and lubricates the food and prepares it for passage, and the tongue pushes the food backwards (Figure 2). Next the the palate raises to close the nose, and the food sits on the back of the tongue prepared for the next step (Figure 3). At this point the most complex process starts: the food sits above the level of the Trachea (breathing tube) and Esophagus (swallowing tube), and the food has to be maneuvered into the esophagus without any of it accidentally spilling into the breathing tube and causing blockage or infection (pneumonia).
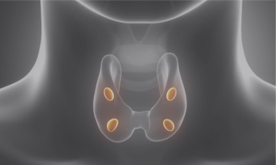
This task is accomplished by the voice box; the voice box sits on top of the breathing tube. It feels the food in the throat and rises up to push against a flap called epiglottis to close itself and the breathing tube, and prevents spillage of food and liquids into the breathing tube (Figure 4). At the same time a very crucial step happens, which is the opening of the valve above the esophagus to accept the food into the esophagus and direct it down to the stomach; this valve is called the upper esophageal sphincter (UES) and the muscle that wraps around the top of the esophagus to create this valve is called the Cricopharyngeus Muscle. The cricopharyngeus muscle is attached on both sides to the Cricoid cartilage which is shown as a grey ring around the Trachea in the image above. It normally is contracted and tightly closes the opening into the esophagus, that is why it acts like a valve. Once the food has passed the UES and is in the esophagus,
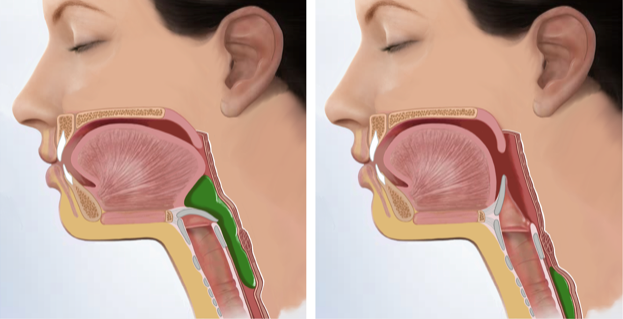 rhythmic movement of the muscles (peristalsis) pushes the food down to the stomach (Figure 5). Coordination between these steps is very important for having an effective and efficient swallow. Without thinking we swallow very smoothly hundreds of times a day. (Figures 2-5)
rhythmic movement of the muscles (peristalsis) pushes the food down to the stomach (Figure 5). Coordination between these steps is very important for having an effective and efficient swallow. Without thinking we swallow very smoothly hundreds of times a day. (Figures 2-5)
Analysis of swallowing problems requires getting a detailed history of the problem, how it started and how it has changed over time. Some problems only affect solid foods (most cases), and others only liquids (usually neurologic causes of dysphagia), and often both. This is followed by a thorough exam that includes a laryngoscopy or an exam of the lower throat. Based on the findings, a variety of tests may then be ordered:
- Video Swallow Study – Under an x-ray, the patient is given different food materials to eat and drink to visualize how the swallow mechanism is working.
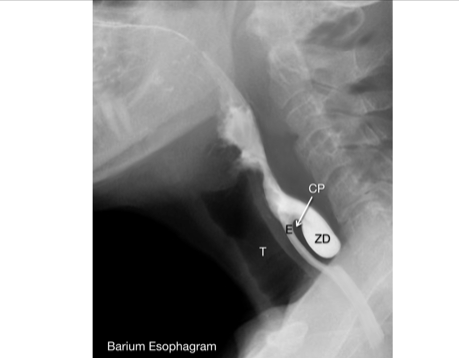
- Barium Esophagram – Under an x-ray, the esophagus is visualized from the UES down to the stomach.
- pH Probe Monitoring – A sensor is placed in the esophagus to measure the amount of acidity.
- Esophageal Manometry – A probe is placed in the esophagus that measures the pressure and sequence of muscle contractions.
- FEESST – Flexible endoscopic evaluation of swallowing with sensory testing to check the swallowing and movement of the vocal cords and throat muscles under direct visualization with a camera. At the same time, the throat’s ability to sense is checked as well.
Causes of Swallowing Problems
- Acid Reflux
- Foreign Material – for example fish or chicken bones.
- Neurologic disorders – causing weakness of the swallowing muscles or lack of coordination.
- Cricopharyngeus Dysfunction – sphincter malfunction that leads to food not passing easily from the throat into the esophagus.
- Zenker’s Diverticulum – Pouch-like sac in the lower throat that collects food and interferes with swallowing.
- Tumors – Benign and malignant tumors of the throat, back of the tongue, voice box and the esophagus can interfere with swallowing.
 Most often found in individuals over the age of 50
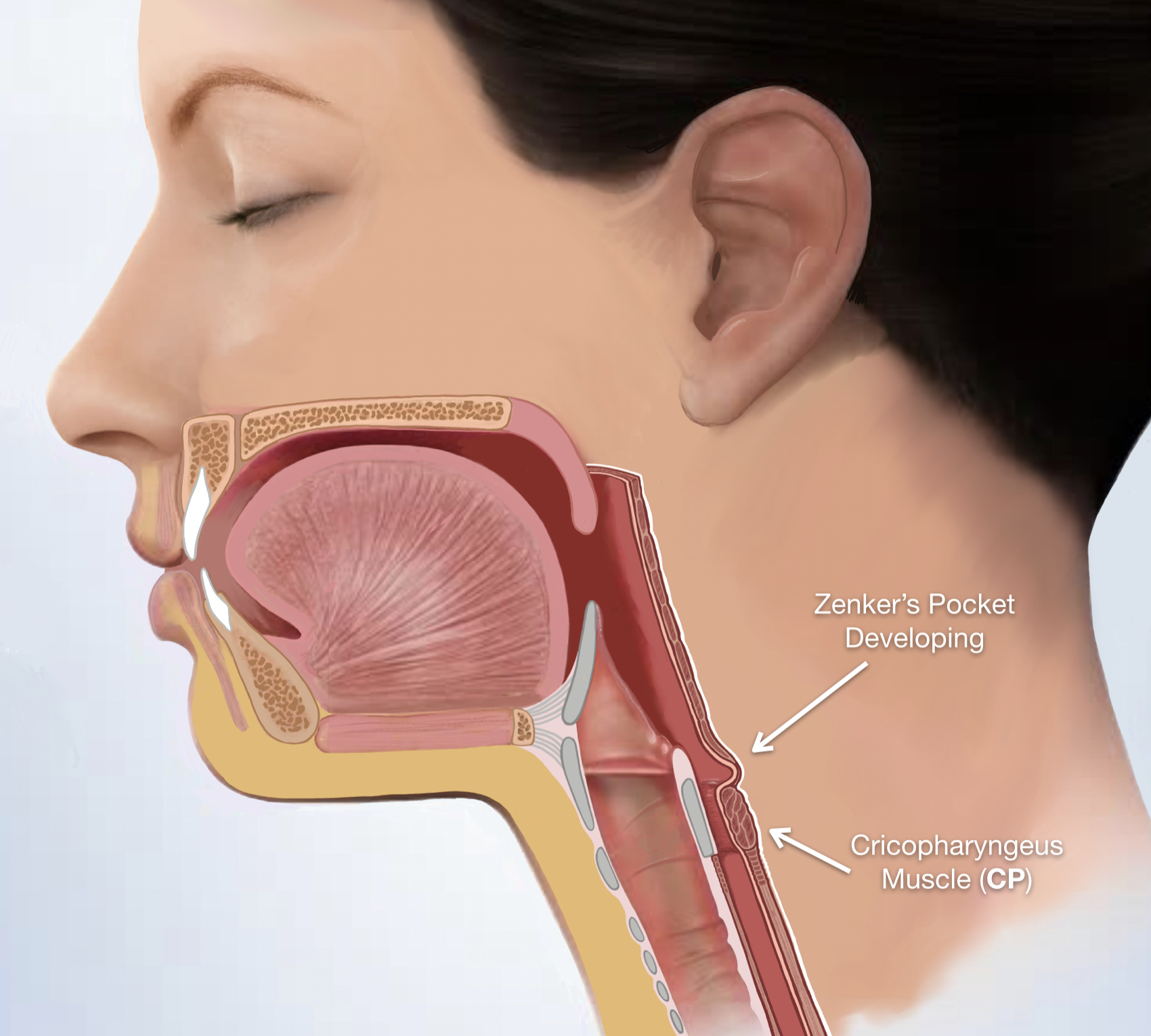
Most often found in individuals over the age of 50  (but possible at even youngerages), Zenker’s diverticulum is a disorder of the throat in which a diverticulum, a pouch, develops in the throat wall. Food may accumulate in the pouch, causing it to fill and at times regurgitate up. Most patients feel food gets stuck in their throat. Pills may also end up inside the diverticulum, making their absorption impossible. The pouch forms because of poorly functioning throat muscles that are not coordinated: the Cricopharyngeus muscle which is a valve at the bottom of the throat does not open when food is being pushed down by the back of the tongue and throat muscles. The throat continually tries to keep pushing the food down so that it can go to the stomach. After this continues for a period of time an area of weakness on the back of the throat starts to bulge out. In time, the bulge grows into a pouch (sac). This pouch is called a Zenker’s Diverticulum (ZD). So ultimately the overactive cricopharyngeus muscle that is not relaxing and opening correctly is the reason for the swallowing issue and the pouch formation.
(but possible at even youngerages), Zenker’s diverticulum is a disorder of the throat in which a diverticulum, a pouch, develops in the throat wall. Food may accumulate in the pouch, causing it to fill and at times regurgitate up. Most patients feel food gets stuck in their throat. Pills may also end up inside the diverticulum, making their absorption impossible. The pouch forms because of poorly functioning throat muscles that are not coordinated: the Cricopharyngeus muscle which is a valve at the bottom of the throat does not open when food is being pushed down by the back of the tongue and throat muscles. The throat continually tries to keep pushing the food down so that it can go to the stomach. After this continues for a period of time an area of weakness on the back of the throat starts to bulge out. In time, the bulge grows into a pouch (sac). This pouch is called a Zenker’s Diverticulum (ZD). So ultimately the overactive cricopharyngeus muscle that is not relaxing and opening correctly is the reason for the swallowing issue and the pouch formation.
(Figures 6-9)
Zenker’s Diverticulum SurgeryThe objective of the surgery for Zenker’s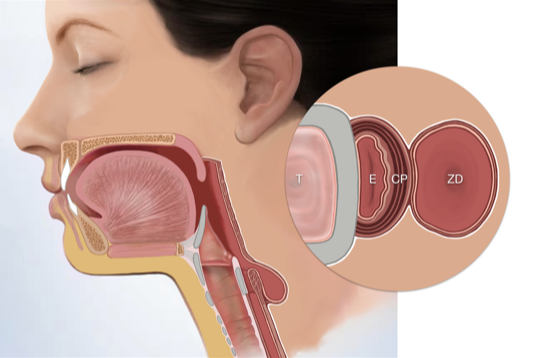 diverticulum is not only to remove the diverticulum, but most importantly to release the malfunctioning muscle of the throat – the cricopharyngeus (CP) muscle.
diverticulum is not only to remove the diverticulum, but most importantly to release the malfunctioning muscle of the throat – the cricopharyngeus (CP) muscle.
Symptoms
At the start the symptoms are mild, and most often the person just experiences mild difficulty swallowing certain foods. Without realizing the person alters their diet and will eat foods that are easier to swallow. This may go on for a while and slowly get worse. Then as the CP muscle gets tighter and the pouch gets bigger, swallowing becomes more challenging, meals take longer, and the person may experience food or liquids collecting in the pouch. They may feel that food regurgitates and comes back up after a short bit of time after eating (usually 20 minutes after a meal). Often the liquid that collects in the pouch keeps coming spilling into the throat and the person feels that they have to always clearing their throat or cough.
These problems continue to progress until ultimately the diet becomes very limited and the person starts to lose weight. Unfortunately once the CP muscle malfunctions, it never gets better on its own, and it will continually get worse.
How to Diagnose
Seeing an ear, nose and throat doctor is imperative anytime a person is experiencing swallowing issues, because there are many causes of swallowing problems (otherwise known as dysphagia). The doctor will look in the throat (procedure done in the office called laryngoscopy) to make sure there is no tumor or infection causing the problem. But in the process the doctor will get the history of how the problem develops and the symptoms associated with it. This will be followed with doing a swallowing study or a barium esophagram which will show the malfunctioning CP muscle as well as the Zenker’s Diverticulum pouch.
 Causes
Causes
The two main causes of a malfunctioning cricopharyngeus muscle are chronic acid reflux or neurologic problem. Both of these conditions make the cricopharyngeus muscle become less coordinated and not open at a the right time during swallowing. While the rest of the throat is working together and pushing the food down.
Endoscopic vs. Open Neck Surgery For Treatment of Zenker’s Diverticulum
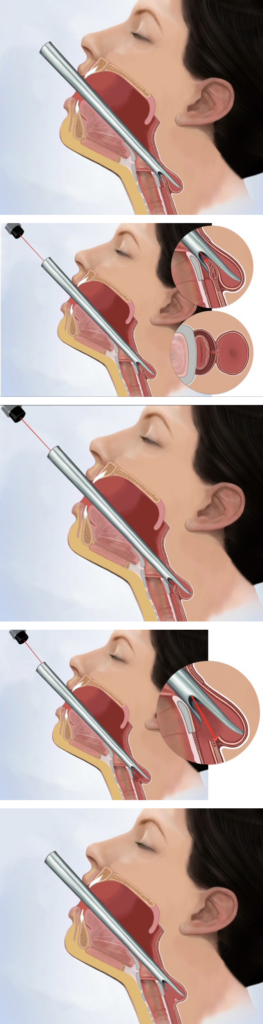
Trans-oral Endoscopic Laser Excision of Zenker’s Diverticulum
Zenker’s Diverticulum SurgeryA special two-prong scope is inserted through the mouth that allows the head and neck surgeon to view the wall separating the esophagus and the diverticulum. This wall contains the poorly functioning cricopharyngeus muscle. The surgeon then uses either a laser or a stapling device to remove this wall, thus uniting the esophagus and thediverticulum.
So there is no cricopharyngeus muscle to get in the way of the food going down into the esophagus, and the pouch is now completely opened into the esophagus so food, liquid or pills cannot sit in it and directly go down to the stomach.
Dr. Larian prefers the laser technique because it is more controlled and precise. The laser cuts the wall that contains the faulty cricopharyngeus muscle one layer at atime, while looking at the area with a microscope and seeing every detail. This allows for accuracy and precision.
Zenker’s Diverticulum SurgeryThe cricopharyngeus is attached on both sides to the back of the Cricoid cartilage which is the grey ring around the trachea in the images shown. By cutting it with the laser the muscle splits apart and no longer can close the esophagus inappropriately. The success rate of this procedure in improving swallowing to a functional level is more then 95%.
Recovery from Endoscopic Laser Treatment of Zenker’s Diverticulum
Recovery from the endoscopic technique is relatively simple. Patients are discharged home the next morning and must follow a liquid diet for one week, then a soft diet for the second week, after which they are able to start a regular diet. Dr. Larian is one of the few surgeons in the country with extensive experience in performing this endoscopic procedure.
 The Open Method
The Open Method
The open technique is used only very rarely, in exceptional situations. An incision is made on the side of the neck, allowing the surgeon to access the diverticulum and the CP muscle. After the CP muscle is cut, the diverticulum is removed using a stapling device. The patient may drink liquids three days after surgery and resume a normal diet one week later. By using the endoscopic technique Dr. Larian has not had to resort to using the open method since the early 2000’s. Excision of Zenker’s diverticulum is best performed by a surgeon who has extensive experience in treating voice and swallowing disorders.
Cricopharyngeus Muscle Malfunction Without Zenker’s Diverticulum
Cricopharyngeus Myotomy
Some complex swallowing disorders may be caused by a malfunctioning cricopharyngeus muscle (or CP). This muscle forms a ring around the upper esophagus. A properly functioning CP relaxes and opens when swallowing so that food may pass through the esophagus and into the stomach. An obstruction may occur if the CP fails to relax which will cause food to get stuck in throat or to pass slowly. Treatment for this problem is to cut the CP so that it doesn’t get in the way of swallowing. This procedure is called a cricopharyngeus myotomy.
A CP myotomy can be performed endoscopically with a laser in the same way that Zenker’s surgery is performed. Sometimes doctors may choose to inject Botox into the muscle to paralyze it for a few months which is a simpler procedure but only lasting a limited time.