Thyroid Cancer
What is thyroid cancer? Thyroid cancer develops from a single cell in the thyroid gland that has multiple mutations causing it to not have inhibitions. As such the cancer cell continually duplicates and grows, until it is large enough to be seen on ultrasound as a nodule. The rate of growth and the aggressiveness of cancer depends on the type of mutations. The types of mutations determine what type of cancer occurs.
gland that has multiple mutations causing it to not have inhibitions. As such the cancer cell continually duplicates and grows, until it is large enough to be seen on ultrasound as a nodule. The rate of growth and the aggressiveness of cancer depends on the type of mutations. The types of mutations determine what type of cancer occurs.
Types of thyroid cancer
- Papillary thyroid cancer – The most common type of thyroid cancer, papillary thyroid cancer develops from the follicle cells that line the colloid lake, and produce thyroid hormones & thyroglobulin. Although it can occur at any age, it most often happens in women between the ages of 30 and 50. Most cases present at early stages and are very curable with surgery. However, some can present with aggressive variant (Tall Cell, Diffuse Sclerosing, & Columnar Cell Variants) and require more involved treatments.
- Follicular thyroid cancer – Follicular cancers also develop from follicle cells. It is the second most common type of thyroid cancer, and occurs most often in people over the age 50. Hurthle cell cancer is a variant of follicular cancer that can be more aggressive. Follicular cancers are hard to diagnose on needle biopsy, and often will need molecular testing to be done on the biopsy specimen to give more information on likelihood of cancer.
- Poorly differentiated thyroid cancer – an aggressive type of thyroid cancer that develops from papillary or follicular thyroid cancer.
- Medullary thyroid cancer – Medullary cancer develops from parafollicular cells that produce the hormone calcitonin, as such medullary cancer also produces excess calcitonin. Checking blood levels of calcitonin can help with diagnosis. This type of cancer can run in families, although 75% happen in people without a family history of this type of cancer.
- Anaplastic thyroid cancer – Anaplastic cancer arises from follicle cells also. They occur in the older population. It is a very aggressive cancer but fortunately rare.
Papillary & Follicular Thyroid Cancer at grouped together in a category called Differentiated Thyroid Cancer (DTC). A great majority of thyroid cancers fit into this category. The staging system for the DTC is interesting because it is different based on the age of the person.
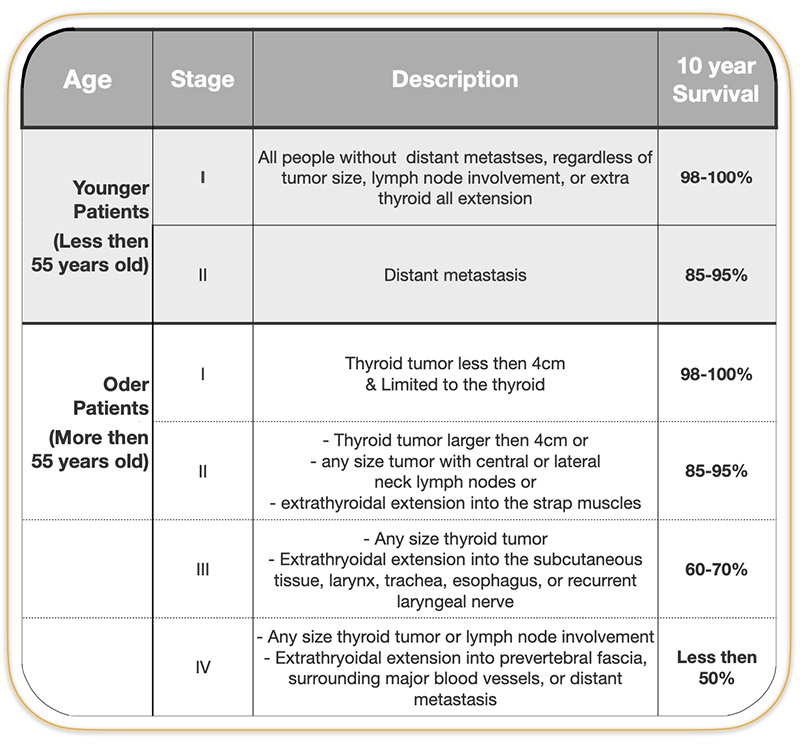
Thyroid Cancer Staging
The staging system for the well differentiated thyroid cancer DTC is described in the chart below and shown in the diagrams that follow it.
Symptoms
Well differentiated thyroid cancers don’t produce any hormone, they do not cause low thyroid hormone production either. The only symptoms they cause is by getting large enough to be felt or press on the surrounding structures such as the breathing tube (causing shortness of breath), swallowing tube (causing difficulty swallowing), or damaging the vocal cord nerve (causing hoarseness).
How To Determine If a Nodule Is Benign or a Cancer
Most nodules are discovered incidentally when a scan is performed for other reasons. Which means that most nodules are found when they are smaller. The following tests can help distinguish between different types of nodules:
- Thyroid blood tests – TSH, Free T3 & Free T4
- Ultrasound
- Needle biopsy
Ultrasound of Thyroid Nodules
The best scan to look at the thyroid and the nodules within it is an ultrasound. It give much more information then other scans including CT scan, or MRI. Based on how a nodule looks on ultrasound, the person performing the ultrasound can categories the risk of the nodule been cancerous. The American Thyroid Association in 2015 created a table that categorizes cancer risk based features of a nodule on ultrasound. Most thyroid surgeons and endocrinologists perform their own ultrasound and are very capable of categorizing the cancer risk of a nodule. And based on that will chose to either to follow the nodule with just ultrasound alone if it doesn’t look suspicious; or perform a biopsy if the nodule looks aggressive or has some features that goes along with a cancer.
CT scans & MRI scans are helpful once the diagnosis of thyroid cancer is made to assess the extent of the cancer and involvement of other structures.
Needle Biopsy or FNA of Thyroid Nodules
Needle biopsy or FNA (fine needle aspiration) is the most definitive way to diagnose what type of thyroid nodule a person is dealing with. It is very simple procedure done in the office of endocrinologists or thyroid surgeons. It involves using the ultrasound machine to locate and visualize the nodule. Once the nodule is clearly seen the skin over it is numbed with anesthetic cream and then anesthetic injection. Then a very small needle is used that can be seen on ultrasound to go through the thyroid gland and into the nodule. As the needle goes through the nodule it scrapes off cells that enter the hollow center of the needle. These cells are then placed on glass slide and sent to the pathologist to look at under the microscope to determine what type of nodule it is. The report of thyroid nodule biopsy is done based on the Bethesda system which clearly categorizes the findings of the biopsy and the risk of malignancy. This allows you and your doctor to make an appropriate decision in regards to the nodule of wether continuing to observe it, or if it is better to remove it.